

R1.63 Pelvic ex-fix
R1.63 Pelvic ex-fix
And how to work around general surgery
Implant Friday 🎉
Let’s hit it.
What I learned today
Most commonly, pins are inserted into the AIIS directed toward the posterior ilium.
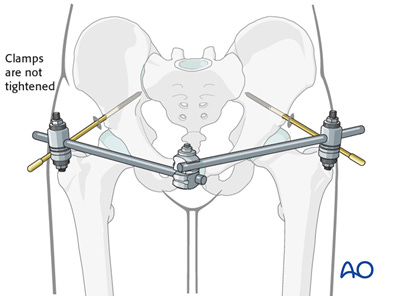
Another option is pinning the iliac crest about 15 mm posterior to the ASIS. This avoids the lateral femoral cutaneous nerve and utilizes the thickest section of bone — the gluteus medius pillar. Haven’t seen this one in person yet during my limited Trauma months.

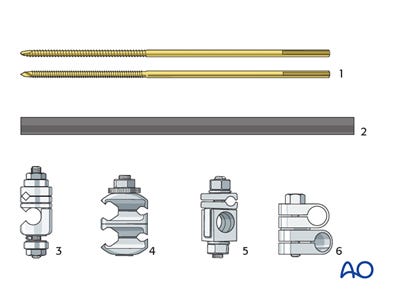
Also, the AO surgery reference has this helpful guide for the names of those ex-fix parts. (I find that when you're the intern, people just hand you things. But soon I'll have to be an actual resident and ask for things by name. That means not saying can you hand me that one thing with the one thingy…)
Okay, sorry for the tangent. On to the actual techniques I wanted to talk about.
Quadrangular anterior pelvic ex-fix
Do you ever run into one of those annoying situations where you finally get a good reduction and put on a beautiful external fixator, only to have the general surgeon undo it?
Apparently it happens. To quote one original snarky figure legend, “This anterior pelvic external fixation device was removed by the general surgeon because it obstructed anterior abdominal access during the laparotomy.”
Say you don't want to delay your ex-fix application until after the gen surg team has finished messing around in there, because that could prolong pelvis-related bleeding. Being orthopedic surgeons, naturally we find our way around this by adding more hardware.

The key to this method is NOT losing the reduction like our general surgery colleagues. The authors recommend using sponges to tightly wrap and tension the iliac pins while the frame is being swapped out.

On Sunday, we’ll get even more fancy… subcutaneous pelvic bridge anyone? Sure, why not.
Sources
AO Surgery Reference - External fixation for acute pelvic treatment
Harborview Illustrated Tips and Tricks in Fracture Surgery 2nd Edition