

R1.5 Osteonecrosis after DDH reduction
R1.5 Osteonecrosis after DDH reduction
Diagnostic criteria and classification
Reasons I created this newsletter: 1) to make myself study every day, 2) to make you study every day, 3) to be transparent about the educational journey as I progress through 5 (okay, 6) years of residency. Today is a day for reason #3.
What I learned today
I thought the main purpose of femoral osteotomy was to perform correction of excessive anteversion and/or valgus. And to facilitate reduction and induce gradual improvement in the acetabulum’s shape, etc.
But apparently, another indication is the prevention of femoral head osteonecrosis. The femur is shortened so that it doesn’t exert excessive contact pressure (leading to osteonecrosis) after a reduction.
Criteria for diagnosing osteonecrosis after reduction:
Failure of the femoral head to ossify (or failure of an already present ossific nucleus to grow) 1 year after reduction
Broadening of the femoral neck
Increased density of the femoral head (followed by fragmentation)
Residual deformity after ossification is complete
There’s even a classification system for this osteonecrosis by Kalamchi and MacEwen (1980). According to the Murphy and Kim JAAOS review, types II and IV are the most relevant (and reported for research purposes).
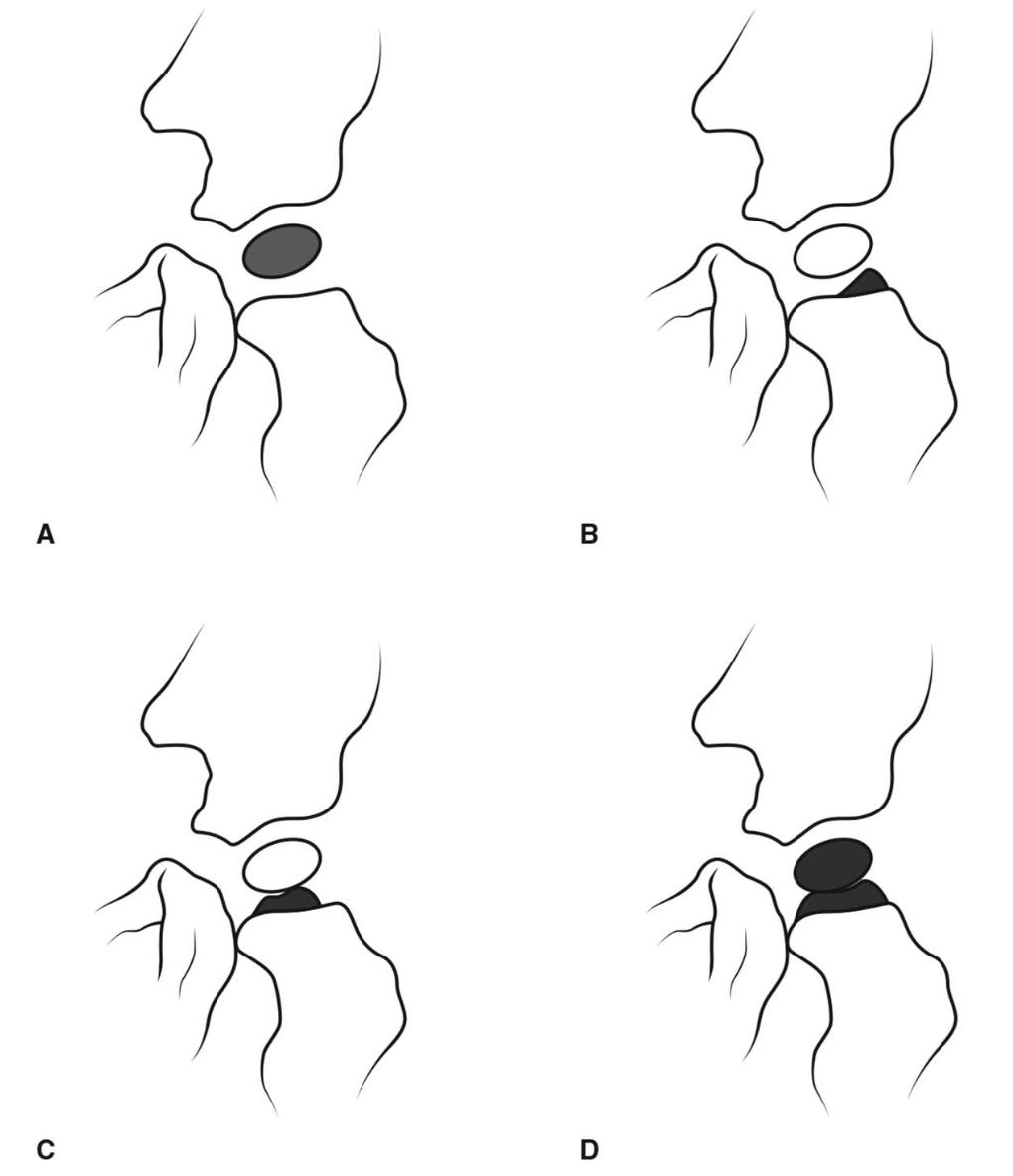
Original figure legend:
Illustrations depicting the Kalamchi and MacEwen classification of osteonecrosis. A, Type I is characterized by alteration in the ossific nucleus. B, Type II consists of lateral physeal damage. C, Type III has central physeal damage. D, Type IV consists of total damage to the head and physis. (Adapted with permission from Kalamchi A, MacEwen GD: Avascular necrosis following treatment of congenital dislocation of the hip. J Bone Joint Surg Am 1980;62[6]:876-888.)
So… uh, yeah. Now I know.
Sources
Murphy RF, Kim YJ. Surgical Management of Pediatric Developmental Dysplasia of the Hip. J Am Acad Orthop Surg. 2016 Sep;24(9):615-24. doi: 10.5435/JAAOS-D-15-00154. PMID: 27509038.